Heart failure and respiratory failure are among the most common causes of hospitalization and death in the United States. In fact, primary or secondary diagnoses of respiratory failure and heart failure accounted for roughly 16% and 25%, respectively, of traditional Medicare hospitalizations in 2018. For most of these hospitalizations, respiratory failure appears as a secondary condition (90.1%) as does heart failure (97.9%). While heart failure and respiratory failure are chronic conditions, patients may be hospitalized with acute exacerbations of these conditions, described as “acute on chronic” conditions. While risk adjustment models to assess provider performance on quality used by the Centers for Medicare & Medicaid Services (CMS) control for respiratory and heart failure, these models do not differentiate acute on chronic from chronic (non-acute).
To better understand similarities and differences in patients with and without acute on chronic conditions, we compared length of stays in a short-term acute care hospital (STACH) and post-STACH use patterns between two groups of patient with heart failure or respiratory failure: (1) Medicare beneficiaries hospitalized with a principal or secondary diagnosis of acute on chronic heart or respiratory failure; (2) Medicare beneficiaries hospitalized with a principal or secondary diagnosis of chronic (non-acute) respiratory or heart failure but without an acute on chronic diagnosis. Our analysis was completed using the 2018 100% Medicare Inpatient Standard Analytic File.
Acute on chronic cases accounted for 34.6% of all heart failure cases in STACHs and 26.0% of respiratory failure cases. Within these cases, acute on chronic hospital stays grouped into a smaller number of MS-DRGs. The majority (75.8%) of all acute on chronic heart failure cases were grouped into 15 MS-DRGs, while roughly a third (35.5%) of chronic (non-acute) heart failure cases fell into the same MS-DRGs. Similarly, 81.5% of all acute on chronic respiratory failure cases fell into 15 MS-DRGs, while 56.2% of chronic (non-acute) respiratory failure cases were grouped to the same MS-DRGs.
Hospital resource use and outcomes for acute on chronic patients also differed from their (non-acute) chronic counterparts. Acute on chronic respiratory failure cases had an average length of stay of 7.5 days compared to 7.0 days for chronic (non-acute) respiratory failure cases (8% difference). Acute on chronic heart failure cases had an average length of stay of 6.6 days compared to 5.4 days for chronic (non-acute) heart failure cases (23% difference).
Discharge disposition also varies across chronic condition types. Our findings show 4.5% of all acute on chronic heart failure cases were discharged to a long-term care hospital (LTCH) compared to 3.6% of all chronic (non-acute) heart failure cases. The difference in LTCH discharges was greater between acute on chronic and chronic (non-acute) patients in the respiratory failure cohort, with 11.2% of acute on chronic respiratory failure cases discharged to LTCHs compared to 7.6% chronic (non-acute) respiratory failure cases. While cases discharged to an LTCH were more likely to be acute on chronic than chronic (non-acute), the reverse pattern was observed for skilled nursing facilities (Heart failure: 60.6% of all acute on chronic vs. 64.1% chronic; Respiratory Failure: 58.8% of all acute on chronic vs. 59.8% chronic) and inpatient rehabilitation facilities (Heart failure: 7.3% of all acute on chronic vs. 9.2% chronic; Respiratory Failure: 6.3% of all acute on chronic vs. 9.4% chronic).
The differences in resource utilization and patient outcomes, identified in this study, suggest that risk adjustment models used to assess provider performance may be improved by distinguishing between these types of heart failure and respiratory failure patients.
Comparison of Average Length of Stay (Days) by Acute on Chronic vs. Chronic (Non-acute) Diagnosis
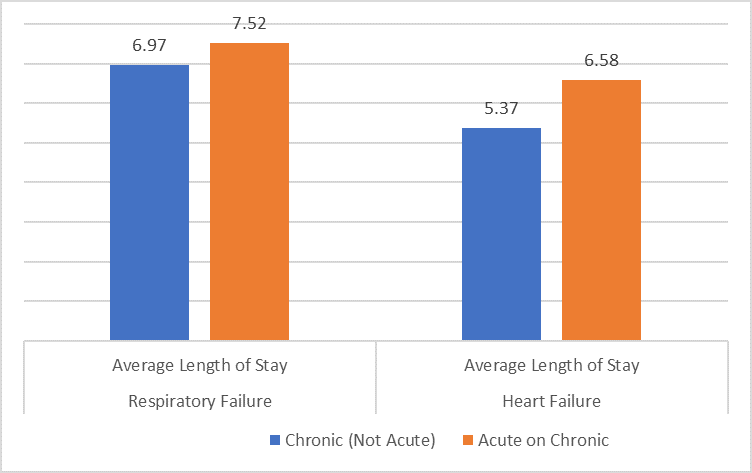
Source: KNG Health analysis of 2018 and 2019 Standard Analytic File.
Services : Blog, Health Economics & Outcomes Research, Practice Area - Evaluation and Health Economics Expertise: health economics, Quality Measurement and Provider Performance

|
Ori Nevo was formerly a Research Associate.
|

|
Marie Steele-Adjognon was formerly a Research Director at KNG Health Consulting. |

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |