As the popularity of Medicare Advantage (MA) plans increased, so did the disenrollment from Traditional Medicare (TM). In previous work, we found that increasing rates of disenrollment from TM accounted for two-thirds (67%) of the growth in the share of MA enrollment between 2019 and 2020. In this blog, we update previously reported disenrollment trends through 2020 with more recent data (2021-2024) and assess rates by different population groups. We separately report findings for Medicare-only beneficiaries and Medicare-Medicaid beneficiaries (dual eligibles), as well as for new Medicare beneficiaries and those who are in the last year of life.
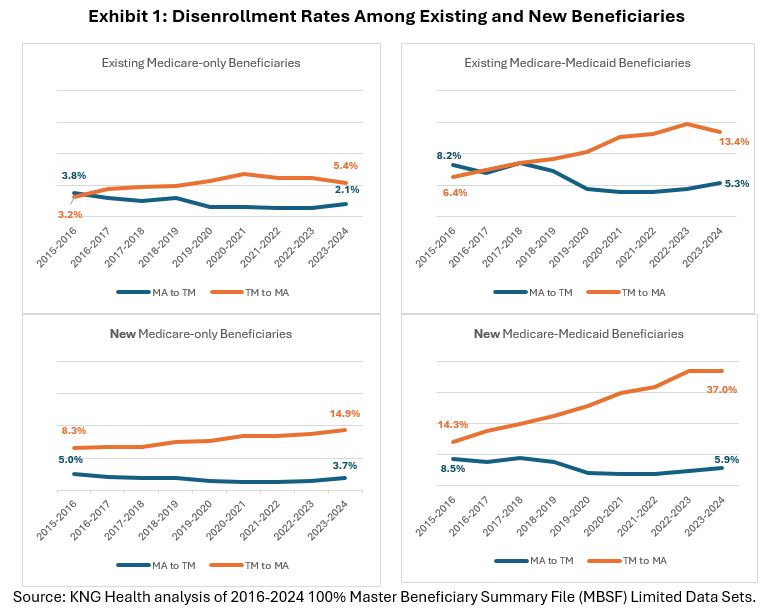
Enrollment in MA continues to increase but at a slower rate due to less disenrollment from TM and more switching from MA to TM. Between 2023 and 2024, disenrollment from TM accounted for 53% of growth in new enrollment in MA, down from 67% between 2019 and 2020. Between 2016 and 2024, the TM disenrollment rate reached its highest point in 2021 at 8.1% and stayed at around the 8% mark until declining to 7% in 2024. The MA disenrollment rate, on the other hand, has increased from 1.9% to 2.7% between 2021 and 2024. In 2024, TM-to-MA switching rates were almost 3 times higher than switching rates from MA to TM (similar to our findings in 2020). However, this reflects a decrease from 2020 for Medicare-only enrollees (2020: 3.7 times higher disenrollment rates from TM-MA vs. MA-TM; 2024: 2.7 times higher) and a small increase for Medicare-Medicaid enrollees (2020: 2.5; 2024: 2.9 times).
Dual eligibles, new enrollees to Medicare, and some minority groups have substantially higher disenrollment rates, especially from TM.
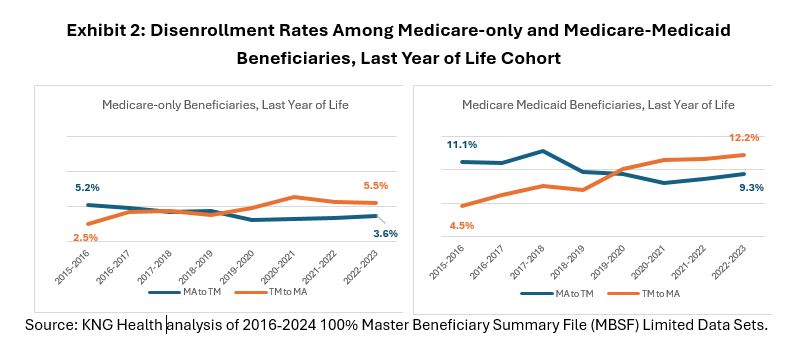
The differential between TM and MA disenrollment rates is smaller for beneficiaries in their last year of life. Since 2020, disenrollment from TM exceeded that from MA for end-of-life beneficiaries but started to converge in 2022 for Medicare-only beneficiaries as rates of switching fell for beneficiaries in their last year of life (from 6.5% in 2021 to 5.5% in 2023) (Exhibit 2).
Conclusion

|
Inna Cintina is a Principal Research Associate in the Evaluation and Health Economics Practice. Dr. Cintina is an applied microeconomist with over a decade of research experience in the area of health economics. At KNG Health, Dr. Cintina is leading evaluations of the impact of managed care on high-need Medicare beneficiaries. Specifically, in work supported by a grant from Arnold Ventures, she is studying the distribution of high-need beneficiaries across enrollment types (Traditional Medicare, Accountable Care Organization (ACOs); and Medicare Advantage (MA)), healthcare services utilization and health outcomes in high-need beneficiaries attributed to ACOs relative to those in MA; and characteristics of MA plans associated with better health outcomes among enrollees. In other work, she studied disparities in utilization of new cardio- and neuro-vascular technologies and impacts of post-acute care settings on beneficiary outcomes. She is an expert in using matching techniques, difference-in-difference methodologies, and other quasi-experimental statistical approaches, as well as producing client-oriented materials, white papers, and manuscripts. She has authored/co-authored more than a dozen articles, which have been published in peer-reviewed journals such as World Bank Economic Review, Health Economics, JAMA, Value in Health, and the American Journal of Managed Care. Prior to joining KNG Health, Dr. Cintina worked at the Lewin Group/OptumServe and the University of Hawaii at Manoa. She has extensive experience in developing and implementing methodologies for identification of causal relationships, advanced analytics, project management, economic burden/cost of illness studies, and impact evaluations of alternative payment models, such as CMMI’s Bundled Payments for Care Improvement Initiative and Oncology Care Model. Dr. Cintina has a PhD in economics from Clemson University, a MSC in European Economics and Public Affairs from University College Dublin, and an MA and a BA in economics from the University of Latvia. |

|
Dr. Lanlan Xu is a dynamic, results-driven health policy executive with over a decade of experience advancing national healthcare reforms in payment and delivery system innovation, Medicare Advantage, and Medicare & Medicaid alignment. She brings proven expertise in health services research, legislative and regulatory strategy, and cross-sector collaboration, and is a recognized leader in advising senior policymakers on value-based care models and healthcare financing reform. Most recently, Dr. Xu served as Deputy Director of the Division of Health Care Financing Policy (HFP) within the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services. In that role, she led a team of economists and policy analysts focused on Medicare and broader health financing strategies, while overseeing ASPE’s Medicare Advantage portfolio. Previously, at the CMS Innovation Center (CMMI), Dr. Xu led evaluations of large-scale health care delivery models, including the Financial Alignment Initiative for dual eligibles and the Initiative to Reduce Avoidable Hospitalizations among Nursing Facility Residents. Earlier in her career at IMPAQ International (now part of AIR), she led Medicare-focused policy research and evaluations, directed the development of care coordination and quality measures, and supported major CMS models and demonstrations. Dr. Xu holds a Ph.D. in Public Policy from Indiana University and a Ph.D. in German Literature from Georgetown University. |

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |