High drug prices are a growing concern among patients and hospitals alike – with the median annual price for new drugs increasing by 35% to $300,000 between 2022 and 2023. The high costs for new drugs create challenges, particularly for those hospitals that rely on Medicare and other government funding sources, which tend to pay below hospital costs. Because Medicare payment rates do not adjust in the initial years after a new drug is introduced, hospitals that provide lifesaving, yet expensive, new drug therapies might incur large financial losses under the inpatient prospective payment system.
Residents of socially deprived communities, as indicated by the Social Deprivation Index (SDI), are more likely to rely on public health insurance options such as Medicare and Medicaid. Hospitals that serve a higher proportion of Medicare and Medicaid patients tend to have lower operating margins compared to those serving higher proportions of commercially-insured patients. As a result, hospitals providing care for lower-income communities may have difficulty providing access to new, high-cost drugs.
The Centers for Medicare & Medicaid Services’ (CMS) New Technology Add-on Payment (NTAP) program provides hospitals with an additional payment to recoup some of the financial losses for drugs (or devices) that are new, costly, and clinically effective. Typically, the NTAP reimburses hospitals either 65% of the cost of the drug or 65% of the money lost in providing care to a patient–whichever is less. The NTAP designation improves the ability of hospitals to provide new drugs to Medicare beneficiaries on an inpatient basis. However, increased reimbursements through NTAPs may not be sufficient to ensure access to new, high-cost drugs in hospitals serving poor communities.
In this blog, we assess the extent to which the adoption of NTAP-designated drugs is similar across communities of varying social deprivation. We report, by a hospital’s SDI, Medicare beneficiaries’ utilization of three NTAP-designated drugs: (1) CABLIVI® – a medication that treats a life-threatening blood disorder; (2) EluviaTM – a drug eluting stent used to treat peripheral arterial disease; and (3) XOSPATA® – a medication used to treat acute myeloid leukemia (AML). These drugs were selected, in part, due to their high prices: the maximum NTAP for these drugs (which represents 65% of their wholesale acquisition costs) ranged from $3,647 (EluviaTM) to $33,215 (CABLIVI®). We identified each drug in inpatient fee-for-service Medicare claims based on assigned MS-DRG and ICD-10-PCS procedure codes. To calculate procedure-specific NTAP utilization rates, we identified inpatient admissions with these procedures and divided that number by the admissions potentially eligible to receive that treatment based on the drug’s therapeutic indication and diagnoses on a claim.
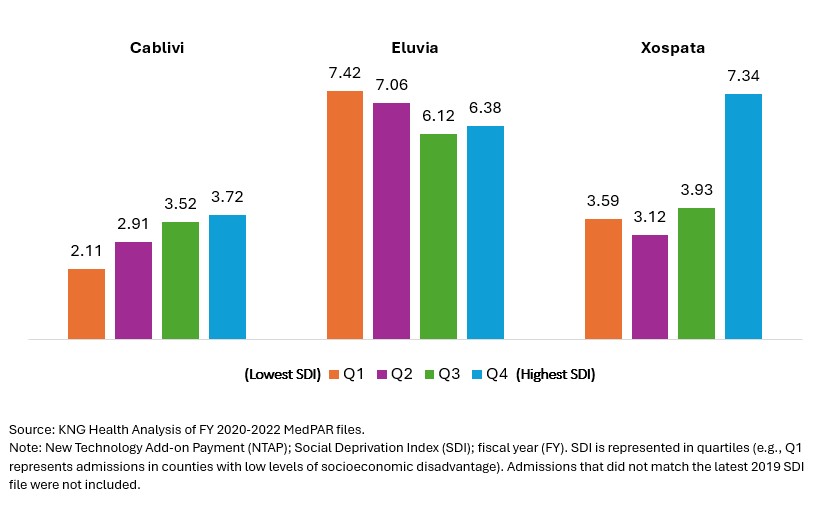
Areas with Higher Social Deprivation saw Higher Utilization of CABLIVI and XOSPATA®, but Lower Utilization for EluviaTM . We found inconsistent utilization rates of NTAP-designated drugs by SDI. XOSPATA’s utilization rate in the highest SDI quartile (i.e., patients treated by hospitals located in the most socially deprived areas) is nearly twice as large as in other quartiles. On the other hand, Eluvia™, the least expensive of the three therapies, has the highest utilization among providers practicing in lower SDI areas.
Utilization Rates of NTAP-Designated Drugs by SDI in FY 2020-22 (per 1,000 Admissions)
Despite the high cost of these new drugs, the observed used patterns do not suggest systematic underuse of selected drugs by hospitals located in areas with high levels of social deprivation. These findings may indicate that additional payments under the NTAP program help support access to novel treatments.
There are several important limitations to the analysis. First, our results may not generalize to other NTAP-designated drugs. Second, MedPAR claims data do not provide all the information needed to establish whether a beneficiary is a good candidate for the drug. Thus, the findings may reflect differences in patient needs across geographic areas. Third, the analysis may not capture patients who have the qualifying condition but have not sought out treatment. Finally, we define SDI based on hospital location and not on where a beneficiary lives. Teaching hospitals, for example, may be more likely to use these new treatments and tend to be located in large, urban areas, but draw patients from many locations.
Services : Blog, Payment Policy & Delivery System Innovation Expertise: Medicare, New Technology Add-on Payment, NTAP

|
Jermaine Piper is a Research Assistant in the Healthcare Reform and Payment Innovation Practice. Mr. Piper’s work focuses on conducting environmental scans on topics such as value-based payment programs, socioeconomic disparities in health care technology access, and financial indicators linked to hospital closures. In addition, Mr. Piper’s work includes data visualization for the construction of health sector chartbooks and quantitative cost-criterion analyses for new technology add-on payment (NTAP) applications for CMS. Furthermore, Mr. Piper also models payment adjustment factors for outpatient prospective payment systems (OPPS) and ambulatory surgical centers (ASC) settings for a state workers compensation program, utilizing proposed and final rules provided by CMS. Prior to joining KNG Health, Mr. Piper worked directly in health care as a Phlebotomist and Medical Laboratory Assistant for a local hospital. In this role, he provided direct patient care and facilitated the running of the hospital’s outpatient clinic and laboratory. Mr. Piper has a Master’s in Public Health with a concentration in Health Policy Analysis and Evaluation at the University of Maryland School of Public Health and has a BS in Public Health from the University of Maryland College Park. |

|
Inna Cintina is a Principal Research Associate in the Evaluation and Health Economics Practice. Dr. Cintina is an applied microeconomist with over a decade of research experience in the area of health economics. At KNG Health, Dr. Cintina is leading evaluations of the impact of managed care on high-need Medicare beneficiaries. Specifically, in work supported by a grant from Arnold Ventures, she is studying the distribution of high-need beneficiaries across enrollment types (Traditional Medicare, Accountable Care Organization (ACOs); and Medicare Advantage (MA)), healthcare services utilization and health outcomes in high-need beneficiaries attributed to ACOs relative to those in MA; and characteristics of MA plans associated with better health outcomes among enrollees. In other work, she studied disparities in utilization of new cardio- and neuro-vascular technologies and impacts of post-acute care settings on beneficiary outcomes. She is an expert in using matching techniques, difference-in-difference methodologies, and other quasi-experimental statistical approaches, as well as producing client-oriented materials, white papers, and manuscripts. She has authored/co-authored more than a dozen articles, which have been published in peer-reviewed journals such as World Bank Economic Review, Health Economics, JAMA, Value in Health, and the American Journal of Managed Care. Prior to joining KNG Health, Dr. Cintina worked at the Lewin Group/OptumServe and the University of Hawaii at Manoa. She has extensive experience in developing and implementing methodologies for identification of causal relationships, advanced analytics, project management, economic burden/cost of illness studies, and impact evaluations of alternative payment models, such as CMMI’s Bundled Payments for Care Improvement Initiative and Oncology Care Model. Dr. Cintina has a PhD in economics from Clemson University, a MSC in European Economics and Public Affairs from University College Dublin, and an MA and a BA in economics from the University of Latvia. |

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |