
The COVID-19 pandemic brought about a drastic downturn in hospital finances at a time when hospitals were called to play a frontline role in the fight against the pandemic. According to projections from the American Hospital Association, hospitals will lose $323 billion in 2020 due to COVID-19, with $202 billion of this loss taking place in the first four months of the national health emergency in the US (March through June). This financial downturn was driven by an unprecedented and abrupt reduction in the utilization of hospital services. As the fight against the coronavirus continues, much remains uncertain. Hospitals’ ability to navigate these uncertain times will depend, in part, on their success in anticipating and responding to future changes in the demand for hospital services.
Below we present a conceptual framework for understanding changes in inpatient hospital services as a result of the pandemic. Our framework suggests the following:
A Conceptual Framework for Forecasting the Effect of COVID-19 on Inpatient Hospital Volume
In examining the effect of COVID-19 on inpatient hospital utilization, it is important to consider how the pandemic affected the demand for inpatient hospital services. In forecasting utilization of hospital inpatient volume during COVID-19, we consider four components of hospital inpatient volume based on admission type.
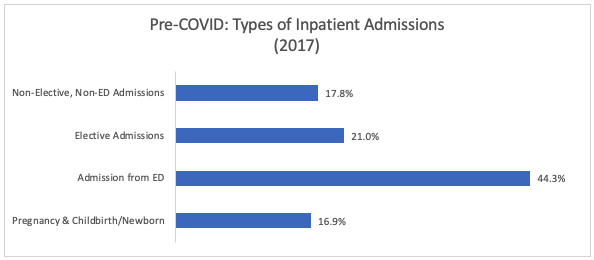
Note: Authors’ analysis of 2017 NIS data. N=4,584 hospitals
Early evidence from select hospital systems shows that in April 2020 hospital admissions were down by up to 35% and surgeries down by up to 70% compared to April 2019. More recently, hospitals are reporting their volumes have climbed back up since the early days of the pandemic, getting closer to pre-COVID levels. A recent analysis of data from 201 hospitals in 36 states showed that all medical admissions declined by 34.1% in April and were still 8.3% below pre-COVID baseline by June/July. These fluctuations in total hospital volume mask substantial variation in volume by admission type. Below, we summarize recent evidence on how COVID-19 affected each admission type.
Hospitals’ pre-COVID mix of inpatient services is a key determinant of the impact of COVID-19 on hospital finances.
Since pre-COVID shares of admissions within each category vary across hospitals, the effect of reduced demand for hospital services due to the pandemic will also affect hospitals differently. Elective hospitalizations make up a relatively greater share of total hospitalizations in small hospitals (26.9%) as compared to larger hospitals (Medium: 14.4%; Large: 15.1%). We observe similar patterns for rural and for-profit hospitals, when compared against urban and not-for-profit hospitals, respectively. Hospitals that rely on a greater share of elective hospitalizations are more likely to be influenced by sharp fluctuations in elective surgeries that occurred earlier during the pandemic. Small, rural, and not-for-profit hospitals also have a larger share of hospitalizations that are non-ED and non-elective relative to other hospitals within its hospital characteristic group. As a result, these hospitals will have a larger impact from long-term shifts in outpatient care and telehealth services on their number of admissions.
Note: Row percentages may not sum to 100% due to rounding. Definition of small, medium, and large hospitals vary by region as indicated in NIS Description of Data Elements.
Future Impact of COVID-19 on Hospital Admissions
There is much uncertainty about how the pandemic will unfold and how hospitals will be impacted as a result in the coming months. Although our medical sector in general and hospitals in particular may be better prepared to weather any new storms related to the pandemic, the incoming flu season is expected to bring new challenges. Even if total hospital volume reaches pre-COVID levels, the distribution of hospitalizations across admission types is likely to change in the long run as a result of the pandemic. The impact on hospital finances will be partially dependent on what the new distribution of hospitalizations across admission types looks like.
Elective Admissions: If there is a jump in COVID-19 cases in the coming months, elective hospital admissions may fall sharply again, potentially due to state executive orders in areas that experience a surge in infections. The long-term impact of COVID-19 on elective admissions will partially depend on patients’ demand for ambulatory care. Furthermore, a recent report from the Commonwealth Fund shows that physician office visits and other ambulatory services have increased since the sharp declines in March and April but have leveled off 10 percent below their pre-COVID volume. This suggests that as hospitals clear the backlog of previously canceled surgeries, the number of elective admissions may also plateau at a lower level than the pre-COVID volume if patients continue to avoid receiving outpatient care in the coming months.
Non-Elective, Non-ED Admissions: The hospitalizations that fall in this category depend on ambulatory care, delivered in outpatient clinics and physician offices. If patients stop going to doctors’ offices for routine or other care, they will be less likely to have hospitalizations that can be scheduled ahead of time and more likely to end up in the ED with potentially more severe conditions. Delayed ambulatory care can reduce hospitalizations in this group and potentially even shift some of these hospitalizations to the admissions from ED.
Admissions from the ED: There will be both upward and downward pressures on admissions from ED in coming months. On one hand, the public’s anxiety over catching coronavirus in the hospital setting may keep ED visits and hospital admissions from ED low. In fact, the magnitude of the decline in ED visits in Spring 2020 coupled with the observation that ED use and hospitalizations fell for acute conditions, such as heart attack and stroke, suggested that part of the reduction in admission from ED was due to people avoiding ED use for conditions that require prompt medical care. On the other hand, heightened sensitivity about coronavirus may increase ED admissions as we head into a new flu season. Furthermore, reduction in routine ambulatory care and elective surgeries may put upward pressure on ED visits as patients delay care until the last minute. For example, many healthcare providers view the term “elective admissions” as misleading because hospitalizations in this category are needed, improve quality of life, and can become “non-elective” urgent hospitalizations if deferred for too long. In the coming months, overall ED use and hospital admissions from the ED will be determined largely by the public’s attitudes towards avoiding prompt medical care and heightened sensitivity towards flu-like symptoms.
COVID-19 has brought about sharp fluctuations in the volume of inpatient hospital admissions. Forecasting future changes in the demand for hospital services and associated changes in hospital finances will be important as we continue the fight against the pandemic. A full accounting of the impact of COVID-19 on hospital finances will require consideration of changes in volume due to the pandemic as well as the payments associated with admission type.
Key Take-Aways

|
Berna Demiralp was formerly a Principal Research Associate at KNG Health Consulting. |
|
|
Aishwarya Agarwal was formerly a Research Associate in the Evaluation and Health Economics Practice at KNG Health. |