Medicare Advantage (MA) plans’ use of prior authorization (PA) – a utilization management tool that requires patients to get their plans’ approval before a service is covered – has drawn scrutiny from numerous outlets, including government oversight organizations, like the Department of Health and Human Services Office of Inspector General and the U.S. Senate Permanent Subcommittee on Investigations. PA is not a novel approach. It has been used by private health insurers for several decades to help contain spending. However, the growth of MA enrollment and use of PA in the program has sparked concerns over the potential negative consequences for beneficiary access to needed care. In this blog, we use MA plan benefits data from the Centers for Medicare & Medicaid Services (CMS) to analyze trends in use of PA for four service types: Mental/Behavioral Health, Therapy Services, Renal Disease Treatment, and Post-Acute Care (PAC). For each service, we report the share of MA enrollees subject to and plans using PA in 2018 and 2024.
Between 2018 and 2024, the percentage of MA enrollees subject to PA increased significantly across all services examined, growing from between 18 and 29 percentage points (Cardiac Rehabilitation and Home Health, respectively).
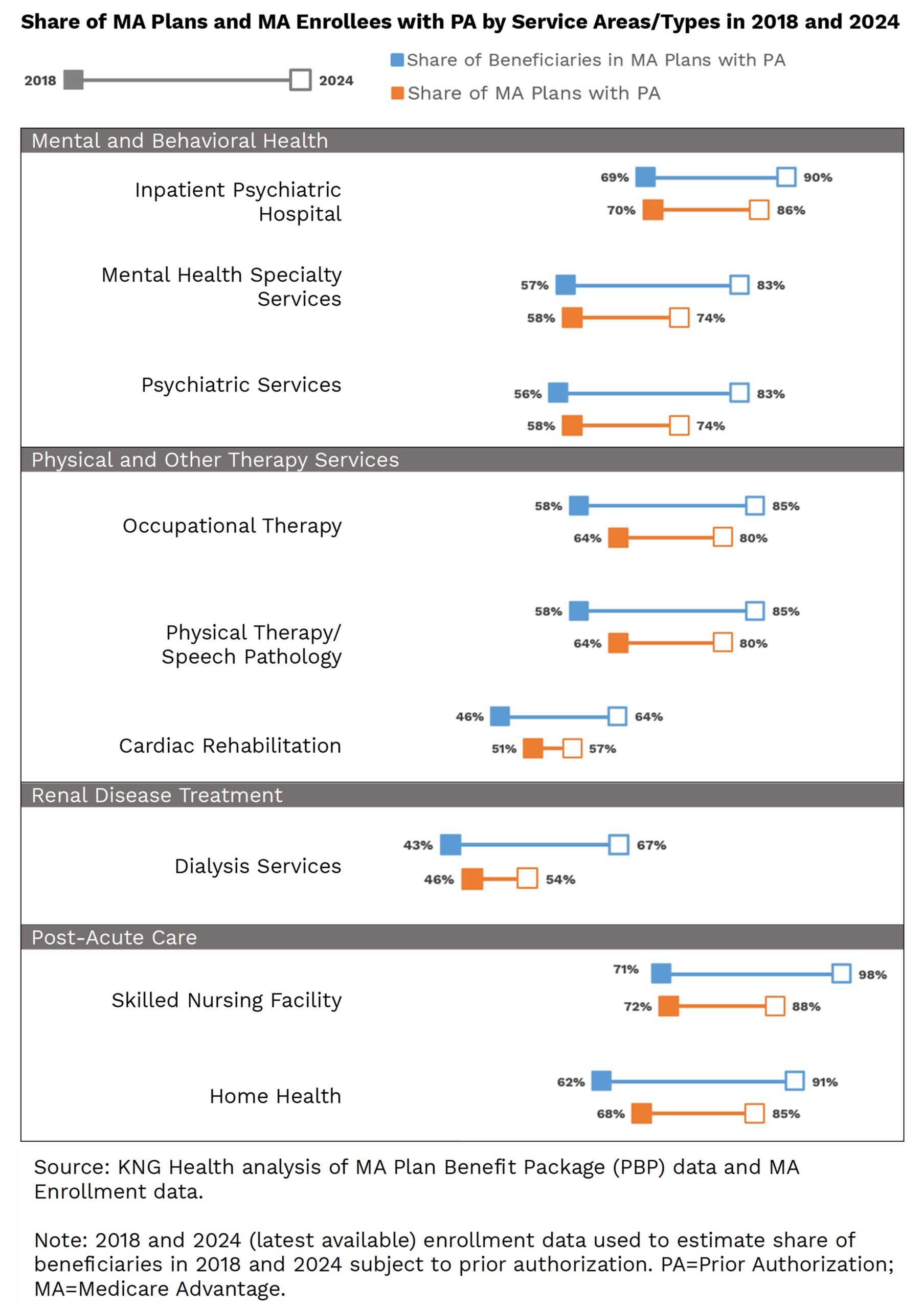
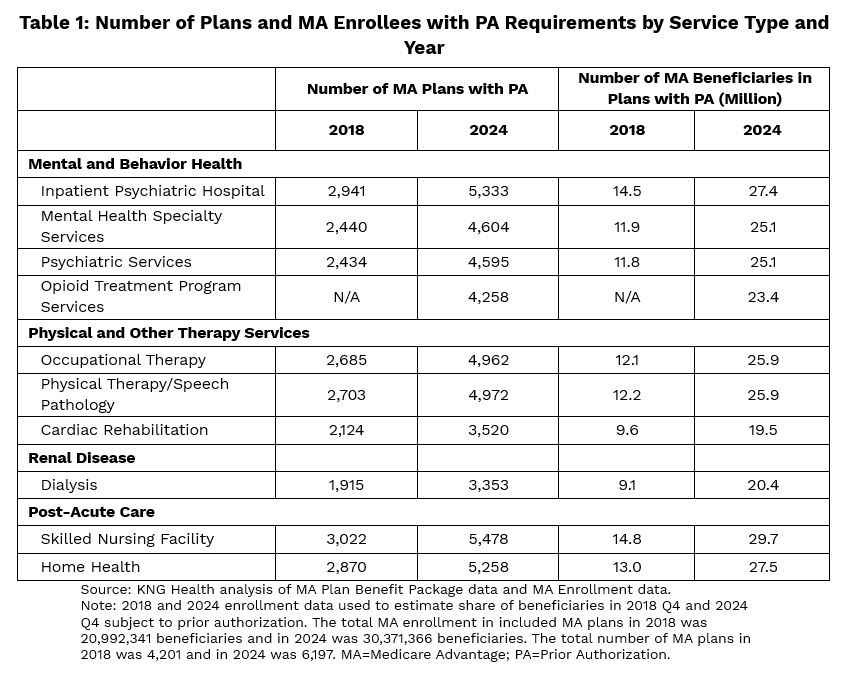
For Mental/Behavioral Health, the share of beneficiaries in plans with PA is around 90% for Inpatient Psychiatric Hospital in 2024 and 83% for other outpatient Mental/Behavioral Health services. Among Physical and Other Therapy Services, PA requirements are relatively high for Occupational Therapy and Physical Therapy/Speech Pathology. In 2024, 85% of MA enrollees are subject to PA for these therapy services, while 58% of MA enrollees needed PA approval for therapy in 2018. Conversely, Cardiac Rehabilitation has one of the lowest PA shares (51% of plans in 2018 and 57% in 2024). The share of plans with PA for dialysis is also relatively low and grew 8 percentage points between 2018 to 2024 (only the percentage of plans requiring PA for Cardiac Rehabilitation grew slower). The share of MA enrollees subject to PA on dialysis, however, increased by 24 percentage points. Finally, while increases in PA requirements were observed across all service types, PA requirements for PAC grew the most. In 2024, 98% of MA beneficiaries are in plans requiring PA for care in Skilled Nursing Facilities, and 91% are in plans requiring PA for home health care: these increases represent at least an additional 14.5 million MA beneficiaries relative to 2018 (Table 1).
Implications
More MA plans are requiring PA for a variety of services, with 99% of MA enrollees subject to PA for some services. Currently, more than half of all Medicare beneficiaries are enrolled in an MA plan (54% or 32.8 million), and this number is projected to grow. While PA may reduce unnecessary care and medical costs, the widespread and growing use of PA increases administrative burden for providers, as care providers are forced to devote time to completing PA authorization forms on behalf of their patients. It also results in delays in care and may result in denials of medically necessary care.
In 2022, there were more than 46 million PA requests (or 1.7 per MA enrollee) of which 7.4% were denied. Denial rates, however, vary across MA plans and types of service. While few (~10%) beneficiaries and their providers appeal initial denial decisions, more than 80% of these appeals are overturned by the MA plans. This suggests that some of the initial denials may have been inappropriate.
The tradeoff between the benefits and costs of PA is an important consideration for policymakers but not well studied. While we document trends in PA requirements, we do not know the extent to which these PA requirements restrict the use of medically beneficial services. For example, MA enrollees subject to PA requirements for dialysis grew significantly for dialysis treatment—the only treatment for patients with acute kidney failure while they await a transplant. Such a finding may be concerning, but without specific data on the effects of PA on patient access to dialysis, we cannot know the impact on patients.
Policymakers have taken a few steps to address concerns over use of PA in MA. In an April 2023 regulation, CMS clarified that prior authorization determinations made by MA plans need to align with Traditional Medicare (TM) coverage guidelines to ensure equal access to treatment for beneficiaries in TM and MA. In addition, CMS intends to require MA plans to submit data on PA at the service level, which will provide greater transparency on its use by MA plans. These steps may ultimately prove helpful to Medicare beneficiaries as they decide whether to enroll in Medicare Advantage, although the impacts of these efforts need to be monitored to ensure that they are having the intended effects.

|
Daisy Hollifield was formerly a Research Assistant at KNG Health. |

|
Inna Cintina is a Principal Research Associate in the Evaluation and Health Economics Practice. Dr. Cintina is an applied microeconomist with over a decade of research experience in the area of health economics. At KNG Health, Dr. Cintina is leading evaluations of the impact of managed care on high-need Medicare beneficiaries. Specifically, in work supported by a grant from Arnold Ventures, she is studying the distribution of high-need beneficiaries across enrollment types (Traditional Medicare, Accountable Care Organization (ACOs); and Medicare Advantage (MA)), healthcare services utilization and health outcomes in high-need beneficiaries attributed to ACOs relative to those in MA; and characteristics of MA plans associated with better health outcomes among enrollees. In other work, she studied disparities in utilization of new cardio- and neuro-vascular technologies and impacts of post-acute care settings on beneficiary outcomes. She is an expert in using matching techniques, difference-in-difference methodologies, and other quasi-experimental statistical approaches, as well as producing client-oriented materials, white papers, and manuscripts. She has authored/co-authored more than a dozen articles, which have been published in peer-reviewed journals such as World Bank Economic Review, Health Economics, JAMA, Value in Health, and the American Journal of Managed Care. Prior to joining KNG Health, Dr. Cintina worked at the Lewin Group/OptumServe and the University of Hawaii at Manoa. She has extensive experience in developing and implementing methodologies for identification of causal relationships, advanced analytics, project management, economic burden/cost of illness studies, and impact evaluations of alternative payment models, such as CMMI’s Bundled Payments for Care Improvement Initiative and Oncology Care Model. Dr. Cintina has a PhD in economics from Clemson University, a MSC in European Economics and Public Affairs from University College Dublin, and an MA and a BA in economics from the University of Latvia. |

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |