Mental health and substance use disorders are common among adults 65 years and older, with an estimated 6.5 million experiencing a mental illness and 4.6 million experiencing a substance use disorder in 2023. Both Traditional Medicare (TM) and Medicare Advantage (MA) plans cover basic inpatient and outpatient services for the diagnosis and treatment of behavioral and mental health conditions including:
We assess how access to behavioral health services in MA plans changed between 2016 and 2025 by zeroing in on prior authorization (PA), referral, and cost-sharing requirements. MA plans may also offer behavioral health (BH) supplemental benefits not offered by TM (e.g., 8% of MA plans covered additional days of inpatient psychiatric hospitalization in 2024). However, examination of BH supplemental benefits is beyond the scope of this blog.
Over 60% of MA plans had a PA requirement for outpatient behavioral services in 2016, and that number grew to over 70% of plans in 2025. The growth in PA over time is not unique to behavioral health services: post-acute care services also saw an increase in requirements, as documented in our previous blog. The number of beneficiaries subject to PA for outpatient mental health services increased from 50% in 2016 to 80% in 2025 (Figure 1). Inpatient services, which are more expensive relative to outpatient settings, typically are subject to stricter utilization management efforts. The vast majority of MA plans already required PA since the start of the study period, with 82% of plans having PA for inpatient behavioral health services in 2016 and 87% in 2025 (Not shown). While the increase in the share of plans is only 5 percentage points, the share of affected beneficiaries has increased from 69% to 93% in 2025 (Figure 1).
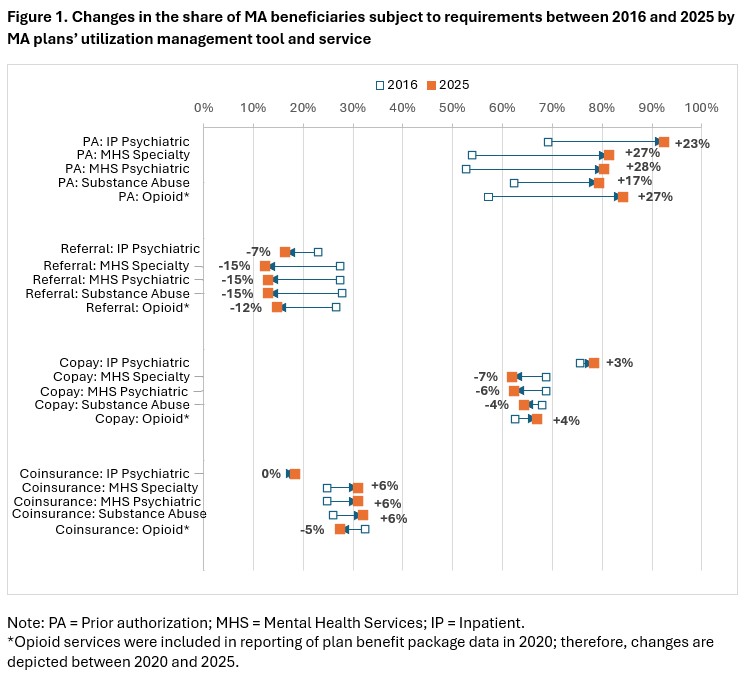
Requirements for a referral became less common over time. By 2026, less than 1 in 5 MA plans required referrals for inpatient or outpatient behavioral health services. This reduction may be due to changes in the numbers of Preferred Provider Organization (PPO) and Health Maintenance Organization (HMO) plans over time. There has been growth in the number of PPO plans and their relative share of the market. PPO plans, unlike HMO plans, do not require referrals.
Share of MA plans with coinsurance and copays has changed little over time. The lack of large shifts could indicate that cost-sharing requirements are not a service-specific choice but, rather, are set by the plans for a whole package of services, with few adjustments over time. One should keep in mind that some MA plans indicated that they have cost-sharing requirements for behavioral services, but the actual requirements were 0% coinsurance or $0 copay. While the number of such plans was small in 2016, by 2025 the number of plans with $0 copayment requirements for outpatient mental health specialty services, outpatient psychiatric services, and outpatient substance abuse services had increased substantially. For example, 55% of MA plans indicated copayment requirements for psychiatric services in 2025, while only 40% had it set above $0 (ranging from $5 to $70 per visit). This trend could potentially reflect the effects of rebates and quality bonus payments received by MA plans, which are mandated to return these dollars to enrollees. For example, in 2025, plans projected using more than one-third of these funds to reduce cost sharing.
Policy Relevance
Treatment for mental health and substance abuse disorders can help beneficiaries manage their symptoms, reduce emergency department (ED) visits related to acute mental health episodes, take control of their substance use, and improve their quality of life. We showed that, over time, some restrictions have relaxed (i.e., referrals and copay), which could improve access to care in Medicare Advantage. However, there is evidence of limited access to behavioral health services, especially in MA. Access limitations are likely created, in part, by PA requirements, as our analysis shows that referrals are becoming less common. Importantly, there is a shortage of mental and behavioral health providers in the U.S. Low reimbursement may be a factor. Psychiatrists, for example, opt-out of Medicare at a higher rate than other types of clinicians (and those providers that opted out from TM are not allowed to contract with MA plans). There are multiple reasons mental health professionals may opt out from serving Medicare population. These reasons range from low reimbursement to reliance on the strong stream of commercial and Medicaid patients.
Policy makers need a better understanding about where—and if—MA beneficiaries get behavioral and mental health services (i.e., in-network, out-of-network, or forgo care altogether). For MA beneficiaries who are accessing these services, more knowledge is needed regarding the impact of these services on health outcomes and utilization (e.g., Are there fewer acute behavioral health episodes? ED-related visits? Hospital stays? Is there less self-harm, overdose, suicide?). Answering these questions will help to guide formation of policies that foster accessibility and quality of care.
Services : Blog, Payment Policy & Delivery System Innovation, Quality & Performance Measurement

|
Inna Cintina is a Principal Research Associate in the Evaluation and Health Economics Practice. Dr. Cintina is an applied microeconomist with over a decade of research experience in the area of health economics. At KNG Health, Dr. Cintina is leading evaluations of the impact of managed care on high-need Medicare beneficiaries. Specifically, in work supported by a grant from Arnold Ventures, she is studying the distribution of high-need beneficiaries across enrollment types (Traditional Medicare, Accountable Care Organization (ACOs); and Medicare Advantage (MA)), healthcare services utilization and health outcomes in high-need beneficiaries attributed to ACOs relative to those in MA; and characteristics of MA plans associated with better health outcomes among enrollees. In other work, she studied disparities in utilization of new cardio- and neuro-vascular technologies and impacts of post-acute care settings on beneficiary outcomes. She is an expert in using matching techniques, difference-in-difference methodologies, and other quasi-experimental statistical approaches, as well as producing client-oriented materials, white papers, and manuscripts. She has authored/co-authored more than a dozen articles, which have been published in peer-reviewed journals such as World Bank Economic Review, Health Economics, JAMA, Value in Health, and the American Journal of Managed Care. Prior to joining KNG Health, Dr. Cintina worked at the Lewin Group/OptumServe and the University of Hawaii at Manoa. She has extensive experience in developing and implementing methodologies for identification of causal relationships, advanced analytics, project management, economic burden/cost of illness studies, and impact evaluations of alternative payment models, such as CMMI’s Bundled Payments for Care Improvement Initiative and Oncology Care Model. Dr. Cintina has a PhD in economics from Clemson University, a MSC in European Economics and Public Affairs from University College Dublin, and an MA and a BA in economics from the University of Latvia. |

|
Kaylee Scarim was formerly a Research Associate at KNG Health Consulting. |

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |