As we have previously documented, almost all Medicare Advantage (MA) enrollees are subject to prior authorization for post-acute care (PAC) services. MA plans use prior authorization and other utilization management tools to shift patients toward lower cost PAC settings. In 2024, post-hospital use of institutional PAC, such as inpatient rehabilitation and skilled nursing facilities, was 7 percentage points lower for MA enrollees as compared to fee-for-service (FFS).
In this blog post, we take a deeper dive by examining use of inpatient rehabilitation facilities (IRFs) in MA and FFS. We examined trends in use of IRFs and compared rates of discharge to IRFs to rates of discharge to skilled nursing facilities (SNFs). To complete the analysis, we used data from 2018 through 2024 MedPAR files. The analysis was limited to hospitals paid under the Medicare Inpatient Prospective Payment System (IPPS). To identify discharge location, we use discharge destination codes on the MedPAR record. MA discharges were identified based on information-only records required to be submitted by IPPS hospitals. The analysis reported in this blog was previously presented at the American Medical Rehabilitation Providers Association 2025 Fall Conference.
Patients Discharged to an IRF Increased by 17% Between 2018 and 2024
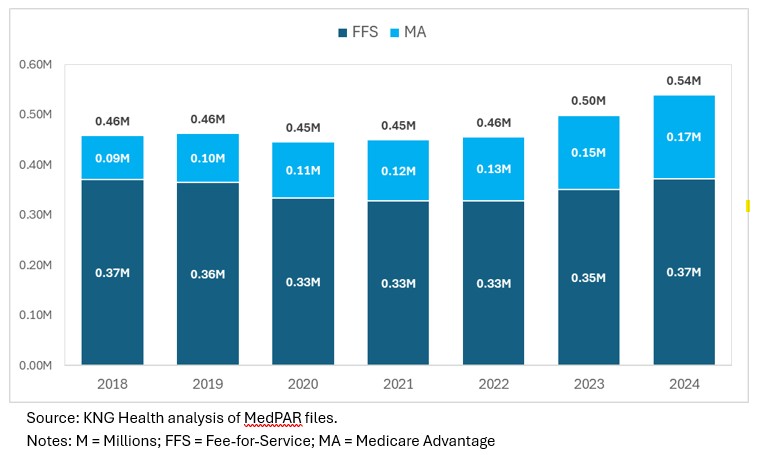
Between 2018 and 2024, hospital discharges to an IRF increased from 0.46 to 0.54 million, an increase of 17% (Figure 1). While the total volume of use in MA grew continually – increasing from 0.9M to 0.17M – FFS volume remained relatively stable with 2024 levels matching 2018 volumes. The stability in FFS volume is noteworthy considering that FFS enrollment fell from approximately 33.6 million to 28.0 million over the same period. Meanwhile, MA enrollment grew from 20 million to 34 million. On a per capita basis, IRF use in MA remained well below FFS levels (1,227 per 100,000 in FFS vs. 468 per 100,000 in MA).
The overall growth in IRF use between 2018 and 2024 can, at least partially, be explained by two factors: (1) between 2018 and 2024, the number of Medicare beneficiaries grew by approximately 10 million (16%), increasing the demand for PAC; and (2) on a per capita basis, MA use of IRFs has grown faster than in FFS (13% vs. 9%).
Figure 1. Medicare Short-term Acute Care Hospital Discharges to an IRF (FY 2019-2024)
MA Enrollees Almost Half as Likely to Receive IRF Care Compared to Those in FFS
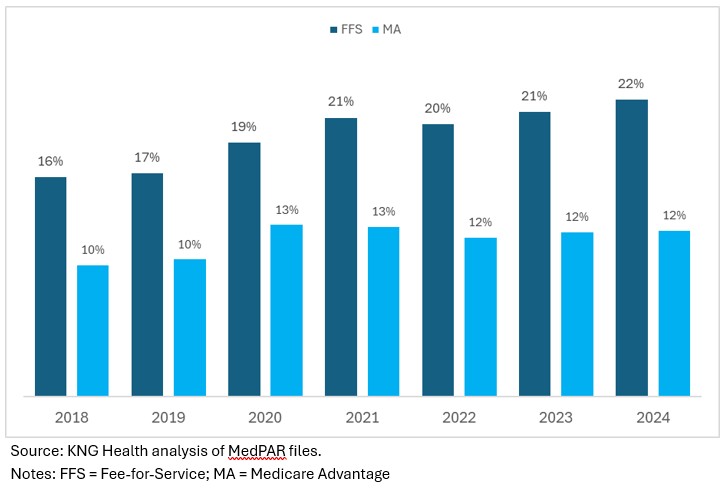
Among patients discharged to either an IRF or SNF, 22% and 12% of FFS and MA patients, respectively, were discharged to an IRF. That is, use of IRFs in MA is approximately 55% the rate of IRF use in FFS. In 2018, corresponding percentages of patients discharged to an IRF were 16% and 10% (indicating IRF use was 62% in MA as compared to FFS) (Figure 2).
Figure 2. Share of Medicare Short-term Hospital Discharges to an IRF (Total Includes IRFs and SNFs)
Medicare Advantage Discharged Higher Complexity Cases to IRFs
For patients discharged to an IRF, we compared the complexity of patients in MA to FFS. We used two measures for patient complexity: (1) number of days in an intensive care unit (ICU) during the IPPS hospital stay prior to IRF admission; and (2) number of comorbidities and complications (CCs) and major CCs as reported on the IPPS hospital record.*
Overall, we found that MA patients discharged to an IRF were more complex than in FFS across all patient types. The average number of ICU days was 3.1 for MA and 4.5 for FFS, while number of CCs and MCCs was 3.7 for MA and 4.1 for FFS. Across conditions, the average number of ICU days prior to IRF admission ranged from 1.0 to 4.9 days for FFS and 1.7 to 6.6 for MA, with the largest difference in ICU days between MA and FFS occurring among patients with lower extremity facture, cardiac conditions, and pulmonary conditions.
Conclusions
Medicare Advantage use of prior authorization results in fewer patients using IRFs in MA as compared to FFS. Previous research has documented improved outcomes for certain patient populations cared for in IRFs but at higher spending. The potential tradeoff between higher spending and better outcomes for patients cared for in IRFs requires additional research and analyses to assess the cost-effectiveness of IRF care for the Medicare population.
Medicare Advantage and its use of prior authorization will continue to be a challenge for IRFs and other PAC providers. Policy makers have grown increasingly concerned on the inappropriate use of prior authorization in MA overall and in PAC. Whether this will result in additional legislative or regulatory activities to rein in MA use of prior authorization is unclear. Regardless, IRF use is likely to continue to grow as the Medicare population increases and ages, with 7.6 million more Medicare beneficiaries expected between 2025 and 2030.
This study has several limitations. First, discharge status codes from short-term acute care hospital records may not always be correct. Second, we identified MA cases from informational-only records in MedPAR. While all IPPS hospitals are required to submit these records, some hospitals may not report a complete set of informational only records.
*Note: We combined the number CCs and MCCs using the following formula: Total CCs and MCCs = # of MCCs + (2/3) * # of CCs. This formula reflects that the additional cost of one more CC is about two-thirds of the cost of one more MCC. This is based on KNG Health analysis.
Services : Blog, Payment Policy & Delivery System Innovation, Quality & Performance Measurement Expertise: Fee for Service, FFS, Inpatient Rehabilitation Facilities, IRFs, Medicare, Medicare Advantage, post-acute care

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |