
Over the past year, the COVID-19 pandemic has ravaged the country and overwhelmed the U.S. healthcare system with overflowing intensive care units (ICUs) and overworked medical professionals. Although short-term acute care hospitals (STACHs) are the nation’s frontline in treating severe COVID-19 cases, the post-acute care (PAC) sector—home health agencies (HHAs), skilled nursing facilities (SNFs), inpatient rehabilitation facilities (IRFs), and long term care hospitals (LTCHs)—has played an important supporting role. Early on in the pandemic, some advocated for an expanded role for LTCHs and SNFs to aid in the response to the pandemic, while others noted that limits in institutional PAC capacity would potentially require greater use of HHAs to address the pandemic. Now, a year into the public health emergency, an examination of Medicare claims data confirms the role that the PAC sector played during the initial months of the nation’s COVID-19 response.
Medicare Post-Acute Care Patterns Shifted Under COVID-19 Pandemic Relative to 2019
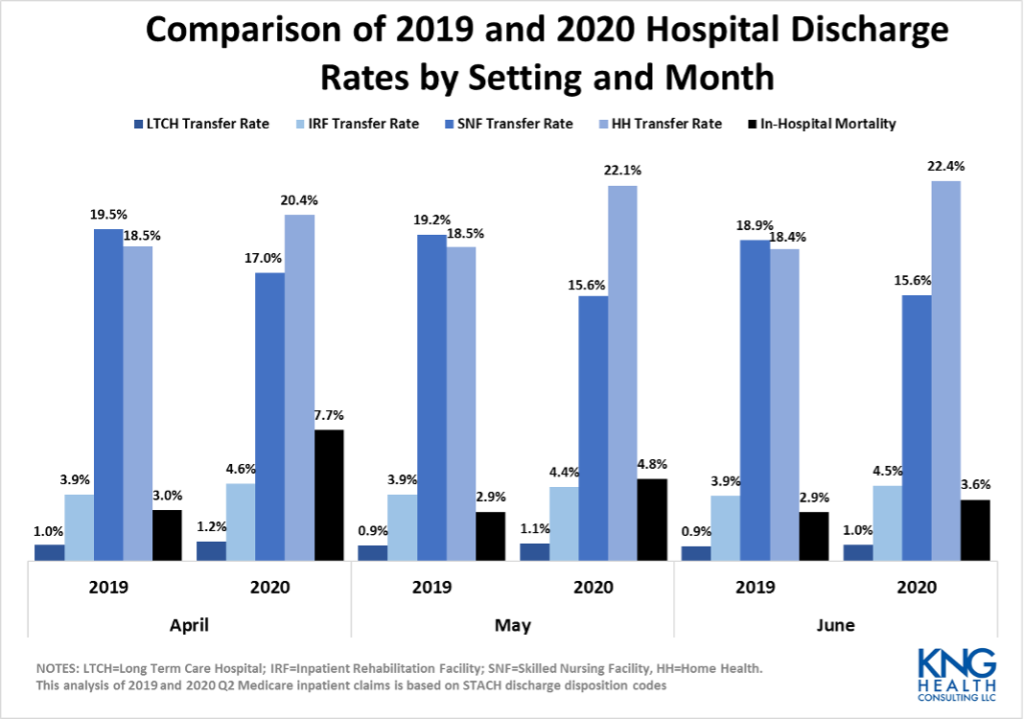
Medicare fee-for-service (FFS) claims data from the first wave of the pandemic (April 2020-June 2020) indicate that PAC utilization patterns shifted, in terms of the distribution of patients across PAC settings and patient mix. Despite an overall decrease in PAC volume, compared to the previous year, the percent of patients transferred from a STACH to a PAC setting increased in the second quarter of 2020. However, a smaller share of STACH patients was transferred to SNFs relative to 2019, while a significantly greater share was discharged with a home health referral. In addition, the transfer rate to LTCHs was almost 4 times higher for COVID-19 patients than non-COVID-19 patients in June 2020. While COVID-19 patients were also more likely to transfer to a SNF than non-COVID-19 patients (twice as likely in June 2020), the opposite is true for patients transferred to an IRF or HHA.
Between April and June 2020, Medicare Volume Was Down and Patient Complexity Was Up in PAC
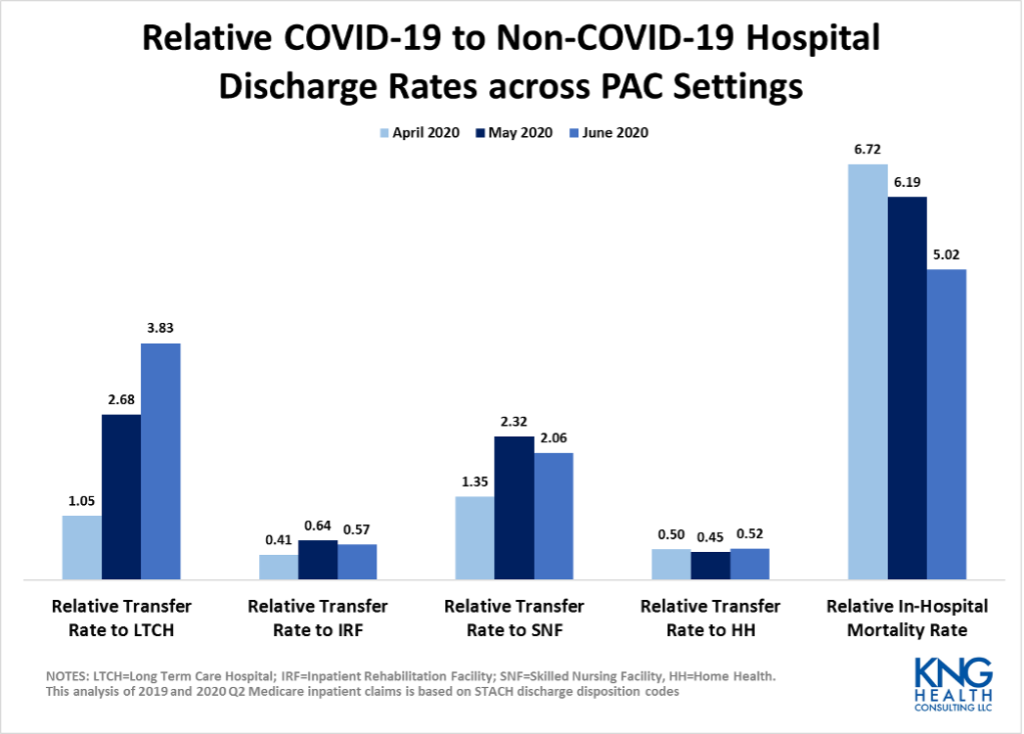
LTCHs and SNFs Shifted their Focus to COVID-19 Patients
The transfer rate of COVID-19 cases to LTCHs and SNFs was significantly higher than for non-COVID-19 cases. In June 2020, a Medicare beneficiary with COVID-19 was almost 4 times more likely to go to an LTCH than a non-COVID-19 patient. During the same period, COVID-19 patients were twice as likely to go to a SNF as non-COVID-19 patients. In contrast, COVID-19 patients were roughly half as likely to go to an IRF or HHA as non-COVID-19 patients. The large differential in likelihood of transferring to an LTCH between COVID-19 and non-COVID-19 patients demonstrates the significant role these specialty hospitals have played during the public health emergency.
Future Work Needed to Gain a Deeper Understanding of PAC Role in COVID-19 Pandemic
At the beginning of the pandemic, the Centers for Medicare & Medicaid Services (CMS) instituted a number of waivers for PAC providers that provided some needed flexibility in responding to the needs of their communities. While our findings should be considered preliminary because it is based on an early release of Medicare claims data, our findings suggest that the waivers had the intended effect of allowing PAC providers to address the pandemic more easily.
Once we get past the acute phase of the pandemic, there will undoubtedly be a thorough assessment of where the U.S. healthcare system succeeded and struggled, with identification of ways to improve the effectiveness and equity of our care delivery systems. That work should include an assessment of PAC. Understanding PAC utilization patterns during the public health emergency may help shed light on the roles of these different PAC providers in caring for Medicare beneficiaries and how those roles can be improved going forward.
[1] Medicare Payment Advisory Commission. A Data Book: Health Care Spending and the Medicare Program. July 2020. Chapter 8 accessed at http://medpac.gov/docs/default-source/data-book/july2020_databook_sec8_v2_sec.pdf?sfvrsn=0
Services : Blog, Practice Area - Evaluation and Health Economics Expertise: COVID-19, Healthcare Cost and Utilization, Medicare, PAC, post-acute care

|
Lane Koenig is President and Founder of KNG Health Consulting and Director of the Healthcare Reform and Payment Innovation Practice. He is a healthcare economist with over 20 years’ experience in the public and private sectors. As President of KNG Health Consulting, Dr. Koenig has overall responsibility for the quality and direction of KNG Health’s research. He serves as Project Director and Principal Investigator for many studies, particularly those related to healthcare reform proposals, healthcare provider payments, value-based purchasing, and delivery system innovations. With expertise on hospital and post-acute care payment and quality issues, his work regularly assesses the potential impact on hospitals and other providers of proposed legislation or regulations. He has assisted both industry and Federal and state governments in the development and assessment of healthcare provider payment policies and value-base purchasing initiatives. Prior to founding KNG Health in 2007, Dr. Koenig was the senior economist in the Office of Policy at the Centers for Medicare & Medicaid Services (CMS). Before joining CMS, Dr. Koenig was a Senior Scientist in the healthcare finance practice at The Lewin Group. Dr. Koenig has led over 100 quantitative and qualitative health policy and health economic studies and has published over 20 peer-reviewed studies in journals, such as Health Affairs, Health Services Research, and Medical Care. He graduated with Honors from the University of Florida, Gainesville and earned his PhD in Economics from the University of Maryland, College Park. |

|
Berna Demiralp was formerly a Principal Research Associate at KNG Health Consulting. |

|
Elizabeth Hamlett is a Senior Research Associate in the Evaluation and Health Economics practice at KNG Health. Ms. Hamlett has extensive experience in project management, the design and implementation of qualitative research (e.g., systematic literature reviews, surveys, and interviews), and in conducting analyses using Medicare inpatient and post-acute care claims data. Since joining KNG Health in 2015, her work has focused on evaluating the efficiency, effectiveness, and value of medical interventions, and supporting the Center for Medicare and Medicaid Services (CMS) Comprehensive Care for Joint Replacement model through learning system activities, such as dissemination of information and data analysis. Ms. Hamlett has experience performing quantitative analyses with a variety of health care data sources, namely Medicare claims and Maryland Health Services Cost Review Commission data. Specifically, she has performed facility-level and condition specific outcome analyses and provided statistical support to multiple pharmaceutical companies in obtaining approval for New Technology Add-on Payments. In addition, Ms. Hamlett has led the design and development of interactive spreadsheet models for multiple projects including the Medicare Payment Advisory Committee’s proposed Hospital Value Incentive Program (HVIP) and CMS State Innovations Model (SIM) Maryland All-Payer Model. She has also performed statistical evaluation of quality measures proposed for inclusion in CMS’ ASC Quality Reporting Program in terms of reliability, validity, feasibility, and interpretability based on data collected through pilot testing for the Ambulatory Surgery Center Quality Collaboration (ASC QC). Prior to joining KNG Health, Ms. Hamlett managed a social psychology laboratory and worked with the non-profit organization, the Dialysis Clinic. Ms. Hamlett earned a Bachelor of Science in policy analysis and management from Cornell University in 2015. |

|
Julia Sheriff is a Senior Research Associate in the Healthcare Reform and Payment Innovation Practice at KNG Health where she conducts quantitative analyses with a variety of healthcare data sources, including Medicare claims data. Ms. Sheriff has conducted analyses to understand the resource needs of Medicare patients with end-stage renal disease. She has also provided support to multiple pharmaceutical companies in obtaining approval for New Technology Add-on Payments. These supplemental hospital payments broaden access to innovative high-value treatments among the Medicare population. Prior to joining KNG Health, Julia was a tenured teacher in the Montgomery County Public School system (Maryland) and Assistant Director of the Peabody Children’s Chorus. Julia earned a Bachelor’s of Music in Piano Performance from the Peabody Institute of the Johns Hopkins University as an award and scholarship recipient. She has earned a Certificate in Data Science from Springboard. She has also completed a Master’s of Applied Statistics/Statistical Science from Colorado State University. |